September 25, 2020; revised April 11, 2022
Patient H.M. provided a critical clue to the role of the hippocampus in memory preservation. Studies on him and a few other patients point to direct and indirect roles played by the brain in preserving memories. The Buddhist and scientific descriptions are the same for habitual (procedural) memory but different for autobiographical (declarative) memory.
Major Components of the Brain
1. The following diagram shows the brain divided into three regions. The following bullet points provide the KEY FUNCTIONS of each area. It is a crude description but provides a simple picture.
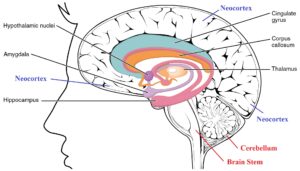
- The cerebellum (indicated in red) controls body movements. The cerebellum also helps with body balance and remembering repetitive tasks. If there is significant damage to the brain stem, one is likely to die. The brain stem controls vital functions like breathing.
- The limbic system plays a vital role in memory. It also deals with emotions. Components of the limbic system are indicated in black.
- The neocortex (indicated in blue) is the largest area of the brain and manages sensory inputs such as vision and hearing. It is also the “thinking brain.” It wraps around the limbic system, starting from the edge of the cerebellum.
Click on the link to download the figure: “Major Components of the Brain.”
Structural Information on the Three Regions of the Brain
2. The above figure shows a brain cut in the middle. Some components of the limbic system have two parts on either side. For example, the hippocampus and amygdala have two identical structures on the brain’s left and right sides.
- On the other hand, the brain stem and cerebellum are single structures.
- In contrast to both, the neocortex has different areas specialized for various tasks. Analysis of sensory inputs happens in the back (visual and auditory cortex.) Parts of the frontal cortex manage planning, speech, and related motor control aspects. The neocortex accounts for 76% of the brain.
Overview of Our Discussion So Far
3. Now, we can better visualize our discussion so far in the previous few posts, especially the post on “Persistent Vegetative State – Buddhist View.” Let us first go over that post.
- The brain stem regulates breathing, heart rate, and blood pressure. Therefore, it is likely that people in vegetative states do not have significant damage to their brain stems.
- The loss of motor control (body movements) is likely due to damage to the cerebellum.
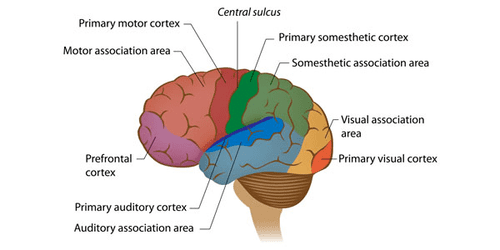
- The visual and auditory cortexes are close to the cerebellum (left figure). Click to download the figure: “Neocortex Areas and Cerebellum.” The limbic system is hidden in this view.
- That roughly matches what we discussed in the previous post about different situations of people in vegetative states. For example, suppose there is damage to the cerebellum area but minimal damage to the visual/auditory cortexes. Such patients may be able to see/hear but not be able to respond.
- On the other hand, if the visual/auditory cortexes and the cerebellum are damaged, the patients will not be able to see or hear as well.
- We discussed those two situations in the previous post.
The Opposite of a “Vegetative State” – Living Without Memory
4. Now, let us discuss a few people who were unfortunate to face different problems due to a third region of the brain located close to the middle of the brain. As we can see from the first figure above, the limbic system lies underneath the neocortex and sits above the brain stem/cerebellum area.
- The limbic system is the “emotional center” of the brain because it controls emotions. It has several components, including the hippocampus, amygdala, and thalamus.
- Our focus here is on the hippocampus. As we will see, it plays a significant role in memory.
- There are two symmetrically-placed hippocampi on either side of the brain. Surgeons removed both of them in a patient who went by the name “patient H.M.”
The account of “Patient H.M.” – Critical Role of Hippocampus
5. Patient H.M. (or Henry Molaison) suffered from frequent bouts of seizures. In 1953, a surgeon removed both his hippocampi in an attempt to solve that problem. Even though the episodes went away, HM suffered a devastating memory loss.
- HM lost the ability to retain NEW memories. But he could remember events up to the operation but could not remember anything for more than a few minutes AFTER the operation. The following video explains it in more detail.
- After extensive studies on patient HM (he died in 2008) and on several other patients with memory loss, neuroscientists have concluded that the hippocampus is the component In the brain that strengthens short-term memories to long-term memories and “passes them over to the neocortex.”
- However, they do not know how those memories can be “passed over to another brain region” or how the brain can keep such “long-term memories” for a long time. In the next post, we will discuss some people’s ability to remember past events extensively. For example, some people can remember what they ate for lunch several years ago on a specific arbitrary date! We will discuss that in upcoming posts.
- The extensive study of patient HM is vital since it allows us to pinpoint one brain component responsible for long-term memories.
Nomenclature of Memory
6. We need to be aware of some standard terms neuroscientists use. That will help us understand the content in the following videos.
- Autobiographical (or episodic, declarative, or explicit) memory is about remembering events, facts, etc. These memories are about dates, events, names, etc. They are the same as nāmagotta in Buddha Dhamma. In Buddha Dhamma, nāmagotta are not in the brain but reside in the “viññāṇa plane.” There is a “transmitter” in the brain that transmits memories to the “viññāṇa plane.” Then, there is a “receiver” in the brain that makes it possible to recall memories from the “viññāṇa plane.” More on that in upcoming posts.
- The other is habitual (or procedural or implicit) memory or being able to do repetitive tasks like playing the piano, riding a bicycle, brushing teeth, etc. They are related to one’s habits. These memories are “hard-wired” in the brain. It appears that the cerebellum in the brain is where such “memory connections” occur.
- Anterograde amnesia is the failure to store memories after trauma. Retrograde amnesia is the failure to recall memories before the trauma. The loss of the hippocampus leads to anterograde amnesia.
Further Details on Patient H.M.
7. The following video is a bit long. But it provides a lot of information.
- @ 4 minutes: Hippocampi on both sides of the brain surgically removed. After that, he couldn’t remember anything that had happened minutes ago. Of course, he could remember events before the operation.
- Imagine the hippocampi to be the “transmitter.” Suppose it transmits new memories to the “viññāṇa plane,” where they remain intact forever. Then, suppose another component (yet unidentified) in the brain can help recall memories. That “receiver” worked for patient H.M. since he could recall memories formed BEFORE removing the hippocampi.
- We will discuss this “theory” in the next post. But keep this in mind as we continue the discussion here.
- @4:40 minutes: “Declarative memory” is the same as the autobiographical memory. “Procedural memory” is the same as “habitual memory.”
- @5:40 minutes: The narrator says there is only one book on patient H.M., But there are two more. See Ref. 1.
8. The Nova clip @7 minutes says that chemical processes create and erase memories. But that is not consistent with either Buddha Dhamma or recent scientific findings.
- @8:40 minutes: The account of H.M.’s medical problems led to surgery.
- @10 minutes: Patient H.M. could remember everything that happened before his operation.
- @10:30 minutes: Dr. Milner concluded that the hippocampus MAKES long-term memories. But we will see that there is a better explanation.
- @11:00 minutes: The drawing experiment showed that he could learn repetitive processes. As we will see below, that comes under “habitual memory” (learning a motor skill) controlled by the cerebellum. But, of course, he had no memory of going through those trial runs of drawing the star.
- @12 minutes: Current scientific explanation of memory formation. This explanation is also consistent with Buddha Dhamma. Construction of “habitual memories” or motor skills appears to occur in the cerebellum.
The Account of Patient E.P.
9. The account of a different person, patient E.P., starts at 4:30 minutes. In 1992, E.P. suffered a viral infection that seemed to have damaged parts of the limbic system. That is very similar to the case of Clive Wearing, which we will discuss below.
- @ 17 minutes: Patient E.P. could not retain memories of events AFTER coming down with the infection. But he remembered events before that. Thus, he does not have autobiographical memories of events AFTER the infection.
- @19:30: The virus destroyed areas around the hippocampus. After that damage, patient E.P. could not retain any NEW autobiographical information. But he remembers everything that happened BEFORE that virus-induced damage. That is similar to the case of patient H.M.
- @22 minutes: The narrator says the hippocampus helps “record the memories.” But as we will see, the hippocampus transmits those memories to the viññāṇa plane.
- @ 24 minutes: Brief discussion of Clive Wearing.
- @25:40 minutes: The account of Dr. Jacopo Annese, who compiles records of the brains of people with different backgrounds, including those with memory problems.
- @30:10 to 32 minutes: The brain of patient H.M. The discussion relevant to our topic stops at 32 minutes.
- @32 minutes to end: Work of Dr. Annese. He plans to make a repository of complete brain scans of 1000 people.
- Next, we discuss a third patient who lost ALL his memories AND cannot make ANY memories.
Clive Wearing – Musician With Seven-Second Memory
10. Clive Wearing was a reputable musician. A herpes virus damaged his brain (around the limbic system) just over a few days in 1985. Unlike patient H.M. and patient E.P., he cannot recall ANY memories. He can remember only those events within the last seven seconds. His situation is even worse than that of the previous two patients.
- Therefore, he cannot recognize anyone. Even though he cannot remember his wife’s name, he knows that she is a special person in his life.
- So, he virtually lives “just at that moment”!
- The following video is a bit long. But it provides a lot of information.
Significant Deductions from Clive Wearing’s Case
11. Note in the beginning that he can play the piano but cannot remember anything that happened even several seconds ago!
- Therefore, his habitual memory is intact (consistent with undamaged cerebellum.) But he has anterograde AND retrograde amnesia, i.e., total loss of autobiographical memory. Therefore, he seems to have lost both the transmitter (hippocampus) and “receiver” (cannot be identified yet.)
- @ 6:40 minutes: He says it is like being dead. No thoughts of any kind except the one that passes by. In that sense, his state is a kind of “vegetative state” even though he can maintain his physical activities.
- @ 9:30 minutes: The account of how he lost memory in several days in 1985.
12. Here are more notable things from the above video:
- @ 10 minutes: How he lost memory within several days. The herpes virus crossed the blood-brain barrier and got into the brain. There is only a one-in-a-million chance of that happening!
- @14 minutes: He says he cannot think about anything. That is why he initially cried all day long. He says it is like being dead.
- @19 minutes: Every moment is the beginning of consciousness! He repeats that at @43 minutes. No thoughts mean like being dead! He was fortunate to be able to play the piano. As we mentioned, such “learned memories” remain hard-wired in the cerebellum. That is a notable difference from “episodic memories,” which are not (and cannot be) “stored” in the brain. We will discuss that in the next post. That is also why he can dress by himself, eat and do other “regular activities” by himself.
13. We can learn a lot about the workings of the brain and the gandhabba by carefully analyzing the accounts of patient H.M., patient E.P., and Clive Wearing.
- We will continue the discussion in the next post.
References
1. Books on patient H.M.: Philip J. Hilts, Memory’s Ghost (1996). Suzanne Corkin Permanent Present Tense: The Unforgettable Life of the Amnesic Patient, H. M. (2013). Luke Dittrich Patient H.M.: A Story of Memory, Madness, and Family Secrets (2017).
2. Book on Clive Wearing: Deborah Wearing, Forever Today (2005).
3. One could Google and find much more information on any of these topics. I have provided just enough material to get the basic idea.
All posts in this section at “Buddha Dhamma – A Scientific Approach.”
